
De Quervain’s Tenosynovitis—a repetitive strain syndrome of the first dorsal wrist compartment—is increasingly common among heavy smartphone users. This condition, involving inflammation of the abductor pollicis longus and extensor pollicis brevis, can significantly impair thumb function and quality of life.
Key treatment strategies often used include:
- NSAIDs or Corticosteroid Injections
- Mobilization with Movement (MVM)
- Tendon Gliding Exercises
- Eccentric and Isometric Loading
- Thumb Spica Splinting – short term immobilization
Winback TECAR accelerates recovery by:
- Reduces local inflammation and swelling by increasing microcirculation and lymphatic drainage.
- Increases soft tissue extensibility and fascial glide, improving tendon mobility and ROM.
- Promotes fibroblast activity, accelerating tissue regeneration and tendon sheath healing.
- Neuromodulates local pain, allowing for improved tolerance during manual therapy or exercise.
- Decreases tissue viscosity, making subsequent mobilization and tendon gliding exercises more effective.
Winback TECAR therapy uses high frequency currents to generate physiological effects on deep tissues without external compression or strain. Operation of two basic modes 1) Capacitative Mode (CET) and 2) Resistive Mode (RET). For De Quervain’s, RET is especially relevant, given the inflammation and thickening in the APL and EPB tendon sheaths and surrounding retinaculum.
Movement Integration with RET Node Application
Position the patient with their forearm resting on the table and the hand slightly off the edge, allowing for unimpeded wrist radial and ulnar deviation.
General TECAR Guidelines
- CET : Return – Forearm flexors resting on the plate. CET handle massage general wrist extensors. Dynamic / Medium / Comfortable warmth 30-40% approximately x 4 minutes
- RET : Return – Forearm flexors resting on the plate. RET handle OR Therapist bracelet. (as described below) Soft / Medium / Comfortable warmth initially 30-40% per length of exercises below.
- Optional: RET progressed to hyperthmia as indicated over the tendon. RET Dynamic / Boost 30-40% intensity (per patient tolerance). More intense heat.
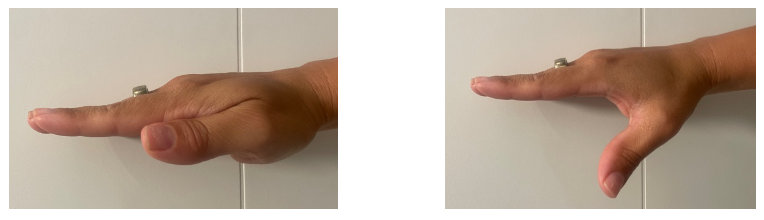
Thumb Extension
Begin by demonstrating and instructing the patient to slowly move the thumb into and out of extension. As they perform this movement, apply the small RET node or use the bracelets and your finger tips over the dorsal wrist compartment, maintaining firm contact. Use gentle linear or circular motions along the inflamed tendons and tendon sheath—targeting the site of De Quervain’s irritation. Perform 10 slow, controlled repetitions.
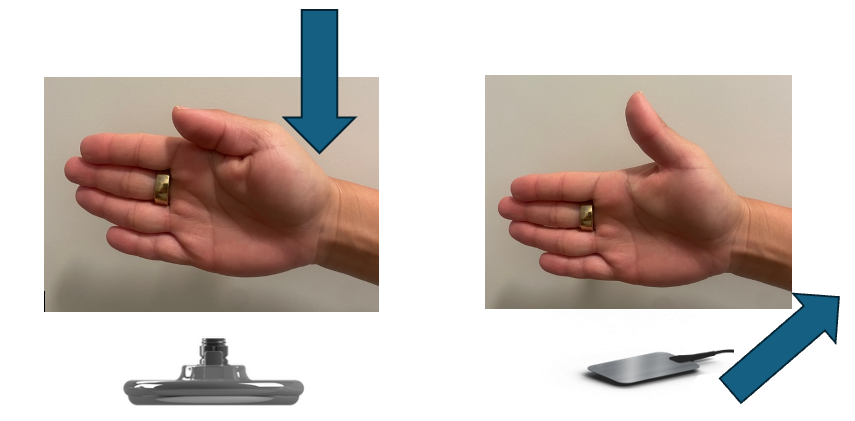
Thumb Abduction
Next, guide the patient through thumb abduction, again for 10 repetitions, while maintaining RET node contact over the same region.
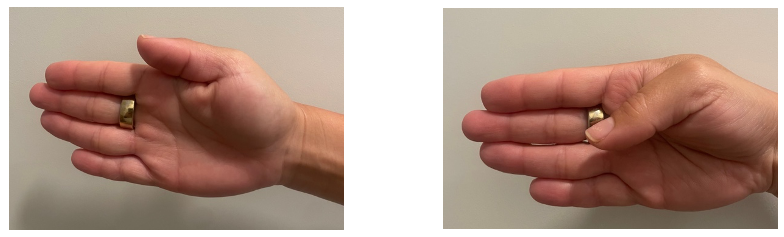
Thumb Flexion
Continue with thumb flexion, encouraging steady movement and mindful control, performing another set of 10.
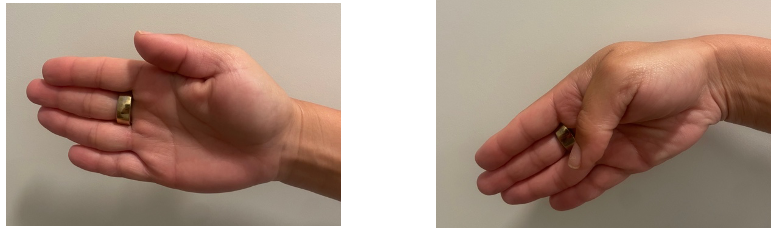
Thumb Flexion with Ulnar Deviation
Finally, instruct the patient to combine thumb flexion with ulnar deviation, staying within their pain tolerance. Repeat this compound motion for 10 additional repetitions.
Throughout the sequence, be aware that movement under TECAR stimulation will increase internal thermogenic activity, resulting in greater tissue warmth and pliability. Monitor patient comfort and tissue response, adjusting intensity and pressure as needed.
While TECAR-specific RCTs on De Quervain’s are limited, evidence from tendinopathy and hand conditions supports its effectiveness:
- Ferrara et al. (2020) reported that TECAR improved outcomes in trigger finger, another stenosing tenosynovitis condition, by reducing inflammation and improving tissue glide.⁽¹⁾
- Ghasemi et al. (2023) demonstrated TECAR’s efficacy in carpal tunnel syndrome for reducing pain and improving nerve function—highlighting its broader impact on musculoskeletal wrist disorders.⁽²⁾
Adjuncts like TECAR can significantly enhance recovery, even in persistent cases without surgery.
References
Al-Bakheet M, Jaradat R, Khresat R, et al. Physiotherapy vs corticosteroid injection as a first line conservative treatment for De Quervain’s tenosynovitis. South Asian J Med Sci. 2020;8(4):1086–1089.



