
Provider Name & Treatment Location: Joseph Giacomo, Hospital for Special Surgery, New York, NY.
Key Words: ACL reconstruction; medial meniscus root repair; medial gastrocnemius spasm; TECAR therapy; diagnostic ultrasound; musculoskeletal ultrasound; semitendinosus allograft; dance rehabilitation
Summary (Abstract)
This case study describes the use of Winback TECAR therapy to treat medial calf muscular tightness in a 61-year-old dancer, 10 months following right ACL reconstruction (semitendinosus allograft) with concomitant medial meniscus root repair. The patient presented with insidious onset of medial calf tightness originating from the mid-muscle belly and traveling to the posterior knee joint capsule, persisting over two weeks coinciding with resumed dance activities.
What makes this case unique within this compendium is the use of diagnostic musculoskeletal ultrasound imaging to objectively confirm TECAR therapy’s physiological effect on muscular spasm before and after treatment. Pre-treatment imaging demonstrated localized hypoechoic or isoechoic nodules within the medial gastrocnemius — consistent with muscular spasm. Post-treatment imaging revealed increased echogenicity over the medial gastrocnemius muscle belly, indicating reduced muscular spasm and increased muscle fiber activation.
The patient completed 2 TECAR treatment sessions over 2 weeks (with ultrasound imaging performed pre and post), followed by 2 additional sessions, and was discharged without lower extremity pain or discomfort. This case provides rare imaging-based evidence supporting the mechanism by which TECAR therapy reduces muscular hypertonicity — a finding with direct implications for the broader case studies in this compendium.
Key take-away lessons:
- Diagnostic musculoskeletal ultrasound provides objective, visual confirmation of TECAR therapy’s effect on muscular spasm: hypoechoic/isoechoic nodules (spasm) visible pre-treatment were replaced by increased echogenicity (reduced spasm, increased fiber activation) post-treatment.
- This imaging evidence supports the proposed mechanism underpinning TECAR’s clinical results across multiple case studies in this compendium — not just subjective pain reduction, but a measurable change in tissue physiology.
- TECAR was effective in a complex post-surgical context: ACL reconstruction with medial meniscus root repair, 10 months post-op, during active return to dance — a population where tissue sensitivity, surgical history, and functional demand intersect.
- A combined passive-then-active TECAR protocol (Deep CET soft tissue mobilization followed by active DL deadlift with concurrent RET-Low adhesive pad setup) addressed both the spasm itself and functional neuromuscular reactivation of the hamstring-calf complex within the same session.
- Resolution was achieved in 4 total sessions (2 with ultrasound imaging, 2 follow-up), with discharge free of lower extremity pain or discomfort.
Introduction
Post-surgical rehabilitation following ACL reconstruction with concomitant medial meniscus root repair involves a complex, phased return-to-activity process. As patients progress toward higher-demand functional activities — such as dance — compensatory movement patterns, altered loading mechanics, and secondary soft tissue symptoms may emerge, even in the later stages of recovery.
Medial gastrocnemius tightness and muscular spasm following lower extremity surgery can contribute to posterior knee discomfort, impaired knee and ankle mechanics, and altered movement quality during demanding activities. Standard management often involves manual therapy, soft tissue mobilization, and progressive loading; however, objective confirmation of treatment effect on the underlying muscular physiology is rarely performed in clinical practice.
This case report is of particular interest within this compendium because it introduces diagnostic musculoskeletal ultrasound as an imaging tool to objectively confirm TECAR therapy’s mechanism of action on muscular spasm in real time — a dimension of evidence that is absent from all other case studies presented here. The pre-to-post ultrasound imaging findings (hypoechoic/isoechoic nodules indicating muscular spasm → increased echogenicity indicating reduced spasm and increased fiber activation) provide direct structural evidence for what the other cases report subjectively: that TECAR therapy reduces muscular hypertonicity and facilitates improved tissue physiology.
Patient Information / Diagnosis
Demographics: 61-year-old patient; dancer (recreational or professional level not specified).
Surgical History: Right ACL reconstruction (semitendinosus allograft) with concomitant medial meniscus root repair. Time since surgery: 10 months at the time of presentation.
Chief Complaint: Insidious onset of medial calf muscular tightness originating from the mid-muscle belly and traveling to the posterior knee joint capsule, persisting over the previous 2 weeks, coinciding with continued resumption of dance activities.
Relevant Medical/Family History: Not specified beyond surgical history above.
Prior Interventions and Outcomes: Not specified in source documentation.
Clinical Findings
Subjective
| Location | Description | Duration | Aggravating Factors |
| Medial calf, mid-muscle belly; posterior knee joint capsule | Muscular tightness; insidious onset; travels from calf to posterior knee | 2 weeks at presentation (10 months post-op) | Continued dance activities |
Objective
Diagnostic Ultrasound — Pre-Treatment Imaging
Musculoskeletal diagnostic ultrasound was performed prior to treatment. Imaging demonstrated localized hypoechoic or isoechoic nodules within the medial gastrocnemius muscle belly. This finding is consistent with areas of localized muscular spasm — hypoechoic regions represent disrupted, poorly organized muscle fiber architecture associated with hypertonicity, rather than the normally bright (hyperechoic), well-organized appearance of healthy muscle tissue.
This imaging confirmed that the patient’s clinical presentation of calf tightness had a demonstrable structural correlate: localized muscular spasm within the medial gastrocnemius, rather than a non-specific or purely subjective symptom pattern.
Detailed Treatment, Timeline, and Outcome
1. Timeline
| Session(s) | Event |
| Sessions 1-2 (over 2 weeks) | TECAR therapy with pre-treatment and post-treatment diagnostic ultrasound imaging performed to confirm physiological effect on medial gastrocnemius spasm. |
| Sessions 3-4 | Two additional follow-up TECAR treatment sessions without repeat imaging. |
| Discharge | Patient discharged without lower extremity pain or discomfort. |
2. Diagnostic Assessment
Diagnostic methods: clinical history and symptom characterization; musculoskeletal diagnostic ultrasound imaging of the medial gastrocnemius (performed pre-treatment and post-treatment during Sessions 1-2) to assess tissue echogenicity and identify hypoechoic or isoechoic nodules consistent with muscular spasm; patient self-report of symptom change.
Diagnosis: localized medial gastrocnemius muscular spasm (confirmed on diagnostic ultrasound: hypoechoic/isoechoic nodular pattern) presenting as calf tightness with posterior knee referral, arising 10 months post-ACL reconstruction and medial meniscus root repair in the context of resumed high-demand dance activities.
Prognostic characteristics: positive prognostic factors included the discrete, localized nature of the spasm (confirmed on imaging), the patient’s functional activity level, and the absence of structural surgical complications at 10 months post-op. Resolution was achieved in 4 total sessions.
Therapeutic Intervention
1. Type of Intervention
Each treatment session utilized a two-phase TECAR protocol: a passive soft tissue mobilization phase followed immediately by an active functional loading phase with concurrent TECAR current. This passive-then-active sequence was designed to first reduce muscular spasm and improve tissue extensibility, then reinforce neuromuscular reactivation and functional loading of the hamstring-calf complex under TECAR current.
2. Protocol Steps
Phase 1 — Passive: Soft Tissue Mobilization
| Setting | Duration | Electrode Setup | Target Area / Goal |
| Deep CET (Capacitive Energy Transfer) — moveable electrode head | 10 minutes | Moveable CET electrode head (active); ground plate strap over distal hamstrings | Medial gastrocnemius; posterior knee region. Goal: reduce muscular spasm, improve tissue compliance, decrease tightness, improve circulation. |
Phase 2 — Active: Functional Loading with Concurrent TECAR
| Exercise | Setting | Intensity | Electrode Setup | Dose | Goal |
| Double-leg (DL) deadlift with 5 lb dumbbells in each hand | RET Low (Resistive Energy Transfer — Low mode) | 40% | Adhesive pad over hamstrings (active); ground rectangular strap over calf | 4 sets of 8 repetitions | Integrate TECAR current during functional hamstring-calf loading; facilitate neuromuscular reactivation; reinforce eccentric control through the posterior chain. |
3. Changes in Therapeutic Intervention
The passive CET phase addressed spasm directly; the active RET phase reinforced neuromuscular reactivation under load and current simultaneously. Diagnostic ultrasound was used after the first two sessions to confirm pre-to-post changes in tissue appearance, providing objective confirmation of treatment effect. Two additional follow-up sessions were completed without repeat imaging, with the patient subsequently discharged free of lower extremity symptoms.
Treatment Protocol and Follow-Ups
Session Frequency / Total Sessions: 4 sessions total: Sessions 1-2 over 2 weeks (with pre/post diagnostic ultrasound); Sessions 3-4 as follow-up without imaging.
Clinician- and patient-assessed outcomes: Diagnostic ultrasound imaging (pre/post echogenicity); patient-reported reduction in overall calf muscle tightness; discharge status (no lower extremity pain or discomfort).
Important follow-up diagnostic and other test results: Post-treatment ultrasound (Sessions 1-2): increased echogenicity over the medial gastrocnemius muscle belly, indicating reduced muscular spasm and increased muscle fiber activation — see Results.
Intervention adherence and tolerability: Patient tolerated the protocol well across all 4 sessions; patient reported reduction in overall tightness following the TECAR sessions.
Adverse and unanticipated events: None reported.
Results after Treatment Completed
Diagnostic Ultrasound — Post-Treatment Imaging
Post-treatment diagnostic ultrasound performed following TECAR therapy sessions revealed increased echogenicity over the medial gastrocnemius muscle belly. This represents a measurable shift from the pre-treatment appearance of hypoechoic or isoechoic nodules (indicating localized muscular spasm and disorganized fiber architecture) toward a brighter, more homogeneous echotexture consistent with reduced muscular spasm and increased muscle fiber activation.
| Measure | Pre-Treatment Finding | Post-Treatment Finding | Clinical Interpretation |
| Medial gastrocnemius ultrasound echogenicity | Localized hypoechoic or isoechoic nodules | Increased echogenicity over the medial gastrocnemius muscle belly | Reduced muscular spasm; increased muscle fiber activation |
Patient-reported outcomes: the patient noted reduction of overall tightness in the right calf muscle following treatment. After 4 total sessions (2 ultrasound-guided, 2 follow-up), the patient was discharged without lower extremity pain or discomfort.
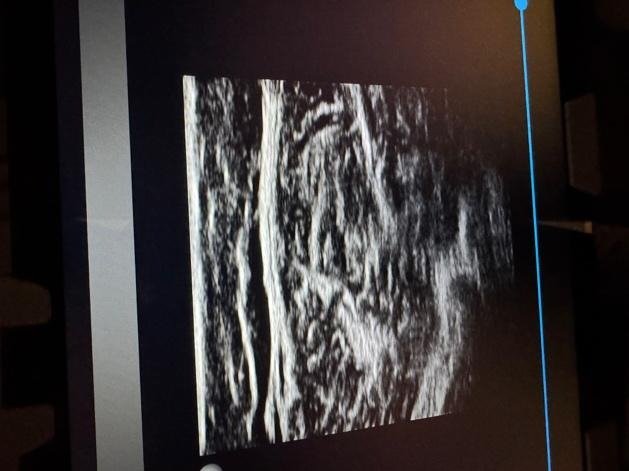
Pre-Treatment
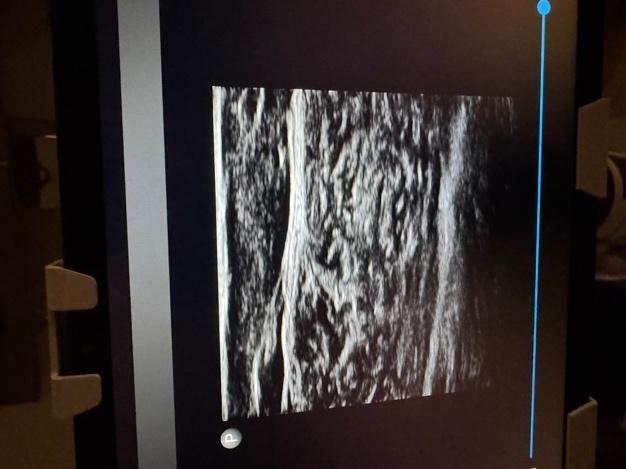
Post-Treatment
Discussion
This case provides an important contribution to the evidence base for TECAR therapy within this compendium: it offers objective imaging confirmation of the physiological mechanism underlying TECAR’s clinically observed effects on muscular spasm — a dimension of evidence that subjective outcomes alone cannot provide.
The pre-to-post ultrasound finding (hypoechoic/isoechoic nodules → increased echogenicity) directly supports the proposed mechanism by which TECAR therapy reduces muscular hypertonicity: through thermal and bioelectric effects that improve circulation, alter membrane permeability, reduce nociceptive sensitization, and restore organized muscle fiber architecture. This imaging evidence provides structural grounding for the symptom improvements reported across the other case studies in this compendium — particularly Cases 2, 5, and 6, which all document TECAR’s application for muscle spasm and guarding, but without objective tissue-level confirmation.
The passive-then-active protocol (Deep CET soft tissue mobilization followed by DL deadlift with concurrent RET-Low adhesive setup) reflects a clinically sophisticated approach: TECAR was used not only to reduce spasm passively, but also to facilitate neuromuscular reactivation under functional load — combining physiological tissue preparation with active rehabilitation in a single session. The choice of DL deadlift is particularly appropriate given the patient’s post-ACL and meniscus-root-repair status and the need to progressively load the posterior chain in a controlled, bilaterally symmetric fashion before returning to the asymmetric demands of dance.
Limitations include the single-patient design, the absence of quantitative echogenicity measurement (the ultrasound findings are described qualitatively), and the absence of follow-up imaging at discharge. Take-away: diagnostic musculoskeletal ultrasound can serve as both a diagnostic tool and an outcome verification method for TECAR therapy, confirming that the clinically observed reduction in muscular spasm reflects a measurable physiological change — not merely a subjective improvement. This supports the broader use of TECAR therapy for muscular hypertonicity across a range of post-surgical and musculoskeletal conditions.
Patient Perspective
The patient noted a reduction in overall tightness of the right calf muscle following TECAR treatment sessions. At the time of discharge (4 sessions total), the patient reported no lower extremity pain or discomfort.